Patent Landscape & Exclusivity
2.1 Key patent filings

Synthesis Route of the Originator
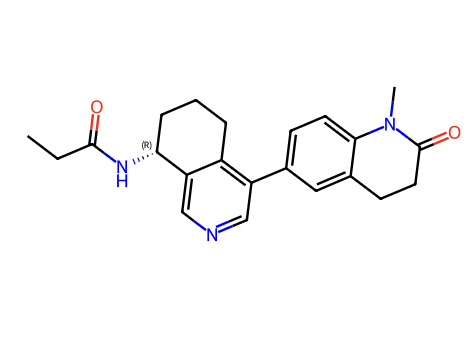
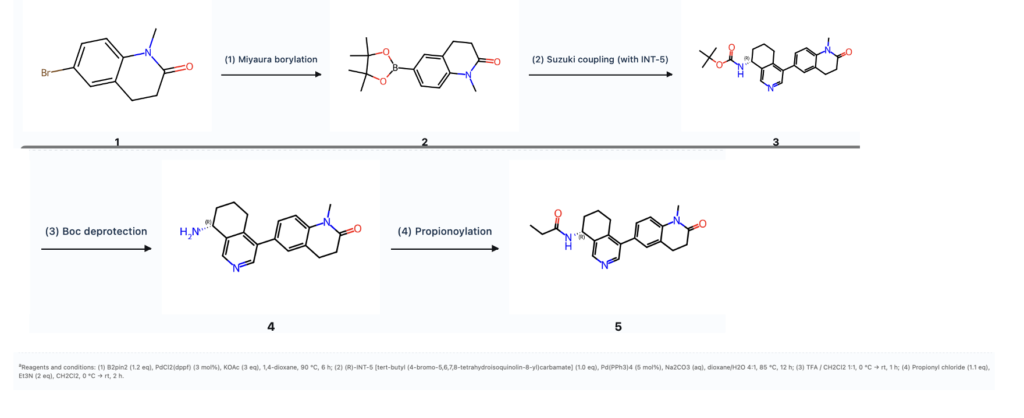
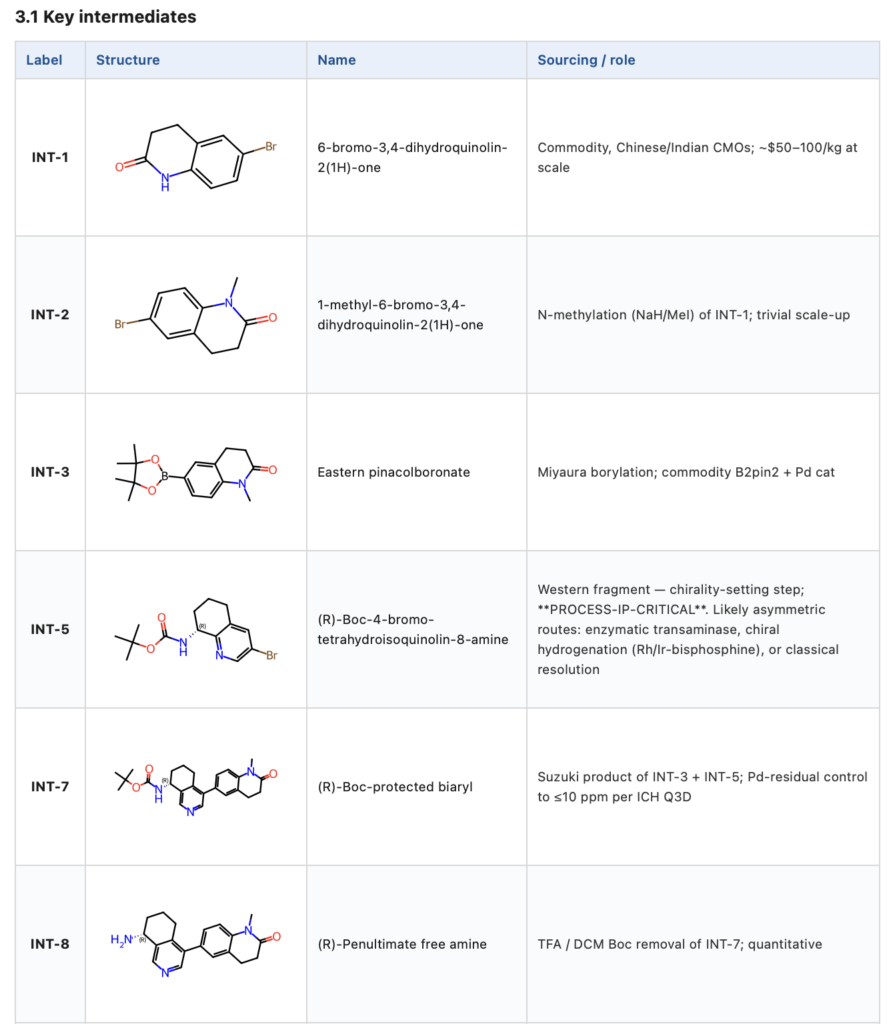
Convergent synthesis disclosed in WO 2014/135561 (Roche). Eastern fragment: 1-methyl-6-bromo-3,4-dihydroquinolin-2(1H)-one (INT-2) → pinacolboronate (INT-3, via Pd/B2pin2 Miyaura). Western fragment: (R)-8-aminotetrahydroisoquinoline scaffold, Boc-protected (INT-5), 4-bromide for coupling. Late-stage convergence: Suzuki C–C coupling at THIQ-C4/DHQ-C6 (→ INT-7), TFA Boc deprotection (→ INT-8), propionoylation with propionyl chloride / Et3N (→ baxdrostat). Chirality-setting step is the key process-IP question; Roche likely uses asymmetric reductive amination or transaminase on the THIQ-C8 ketone (specific route in patent working examples — not yet disclosed in open primary literature).
Key peer-reviewed literature
According to PubMed, the following recent peer-reviewed records are most relevant:
- Qureshi AJ et al., Cardiovasc Drugs Ther 2026 — Baxdrostat and Aldosterone Synthase Inhibitors: A New Class for Treatment-resistant Hypertension (PMID 42126470) — Direct baxdrostat review with updated BaxHTN + Bax24 numbers used in §5.2
- Gallo G et al., Eur Heart J Suppl 2026 — Aldosterone synthesis inhibitors in resistant hypertension: the BaxHTN trial(PMID 42099482) — ASI class review centred on BaxHTN
- Cherney DZI et al., Diabetes Obes Metab 2026 — Effects of Vicadrostat/Empagliflozin in People With Chronic Kidney Disease: Metabolic Subgroup Analyses (PMID 42086479) — Competitor (vicadrostat / BI 690517) Ph2 CKD subgroup data used in §7.4
- Gill OA et al., Dose Response 2026 — Optimal Dose of Lorundrostat in Uncontrolled Hypertension: A Dose Response Meta-Analysis (PMID 42130914) — Competitor (lorundrostat) meta-analysis used in §7.4
- Schnell O et al., Cardiovasc Diabetol 2026 — CVOT Summit Report 2025: advances along the cardiovascular-kidney-metabolic disease continuum (PMID 42092956) — Highlights baxdrostat (BaxHTN) and finerenone + empagliflozin (CONFIDENCE) — CKM positioning
- Parisien-La Salle S et al., Endocrinol Metab Clin North Am 2026 — Evaluation and Management of Primary Aldosteronism (PMID 42067270) — Confirms ASIs as new option for PA — supports §5.2 label-expansion thesis (NCT07007793)
- Todua I et al., Am J Med 2026 — Management of salt-sensitive hypertension in clinical settings (PMID 42103091) — Salt-sensitive HTN as a target sub-population; ASIs noted
- Mohagaonkar S et al., Br J Pharmacol 2026 — Atrial natriuretic peptide counteracts aldosterone secretion by preventing acute angiotensin II-induced… (PMID 42116793) — Mechanistic background — ANP/cGMP/PDE2A pathway opposing aldosterone
5.5 Endpoint landscape across Phase 3 resistant-HTN trials
Across 30 Phase-3 resistant-HTN trials analysed (ClinicalTrials.gov v2 MCP): the canonical primary endpoint is change-from-baseline in seated office SBP at week 12. Secondary endpoints centre on DBP, 24-h ABPM, and the proportion achieving SBP <130 mmHg. BaxHTN’s 2-mg arm (−15.7 mmHg absolute / −9.8 placebo-corrected) and Bax24’s −14.0 mmHg placebo-corrected 24-h ABPM are positioned at the high end of the class.
CMC / manufacturing risk profile
- API DMF holder: Not yet listed at FDA DMF search (typical filing post-NDA approval); monitor for DMF Type II filing 6–12 months post-launch
- Drug product CMO: Not publicly disclosed; likely AstraZeneca internal Macclesfield (UK) site or contract (AZ has historically split internal/external for tablet products)
- KSM supply: Dihydroquinolinone and tetrahydroisoquinoline scaffolds: commodity, Chinese/Indian CMOs
- Critical process risk: (1) chirality-setting step on THIQ-C8 (transaminase or chiral hydrogenation) — IP-protected, hard to second-source; (2) Pd residual control on Suzuki step (≤10 ppm per ICH Q3D); (3) polymorph control of final API
- Estimated API COGs (USD): Back-of-envelope at commercial scale: $1,000–3,000 / kg API (4 late-stage steps + 3 steps each fragment, Pd-catalyzed Suzuki, chiral catalyst). At 1–2 mg dose, <$0.01 COGs per tablet → wide gross margin vs. expected US list price (likely $5–10/tablet)
Pharmacokinetics & metabolism
| Property | Value |
|---|---|
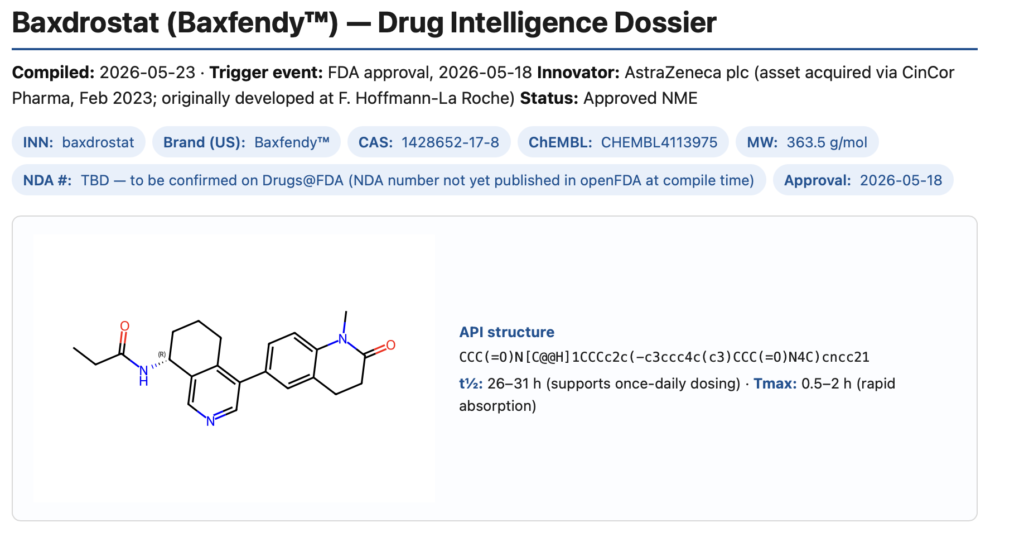
| Half-life (t½) | 26–31 h (supports once-daily dosing) |
| Tmax | 0.5–2 h (rapid absorption) |
| Primary metabolism | CYP3A4 (inferred from itraconazole DDI study NCT06357520; itraconazole = potent 3A4 inhibitor) |
| PD marker (aldosterone suppression) | Plasma aldosterone reduced 51–73% on day 10 of MAD; no meaningful effect on cortisol (selectivity confirmed clinically) |
| Food effect | Minimal expected (no specific food-effect language in BaxHTN protocol); QD oral |
| Hepatic impairment | Likely dose adjustment in moderate–severe (CYP3A4 substrate); specific study pending |
| Renal impairment | Small molecule (MW 363); not dialyzable; expect modest clearance reduction at low eGFR but CKD development program (NCT06268873) ongoing |
| QT/QTc study | NCT06194032 — thorough QT/QTc (Phase 1), negative at therapeutic and supratherapeutic doses |
| ¹⁴C-AME (mass balance) | NCT05961384 — ¹⁴C-baxdrostat mass balance (completed; full report not yet published) |
DDI / interaction flags: – Strong CYP3A4 inhibitors: Ketoconazole, ritonavir, clarithromycin — expect dose-reduction / contraindication language – Strong CYP3A4 inducers: Rifampin, phenytoin, carbamazepine, St. John’s wort — expect reduced efficacy warning – Transporter: MATE1 / MATE2-K inhibition IC₅₀ ~1.3–2.7 µM (per Selleck data) — clinically relevant for metformin renal clearance